Cervical cancer web-based clinical decision support tool
Home Back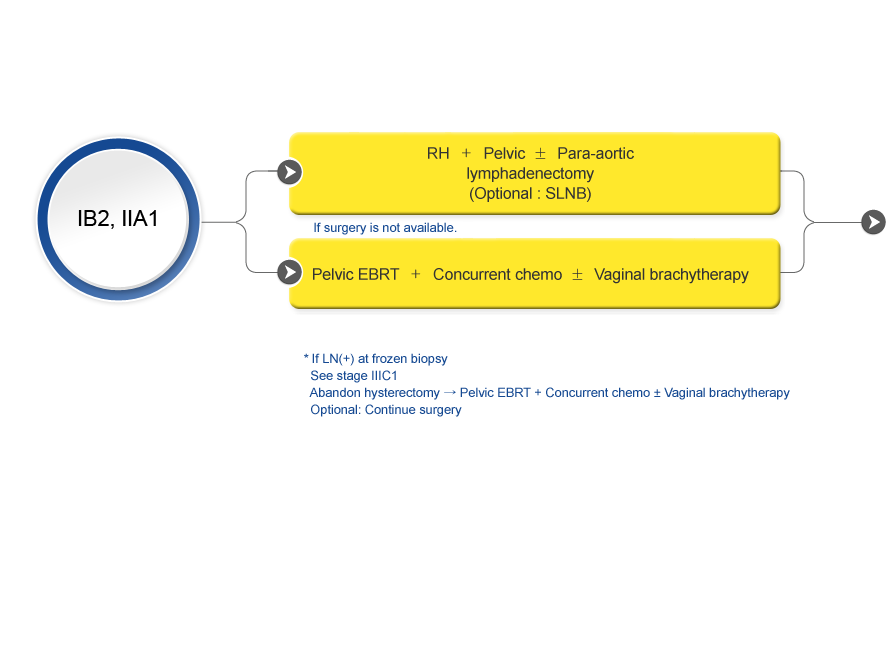
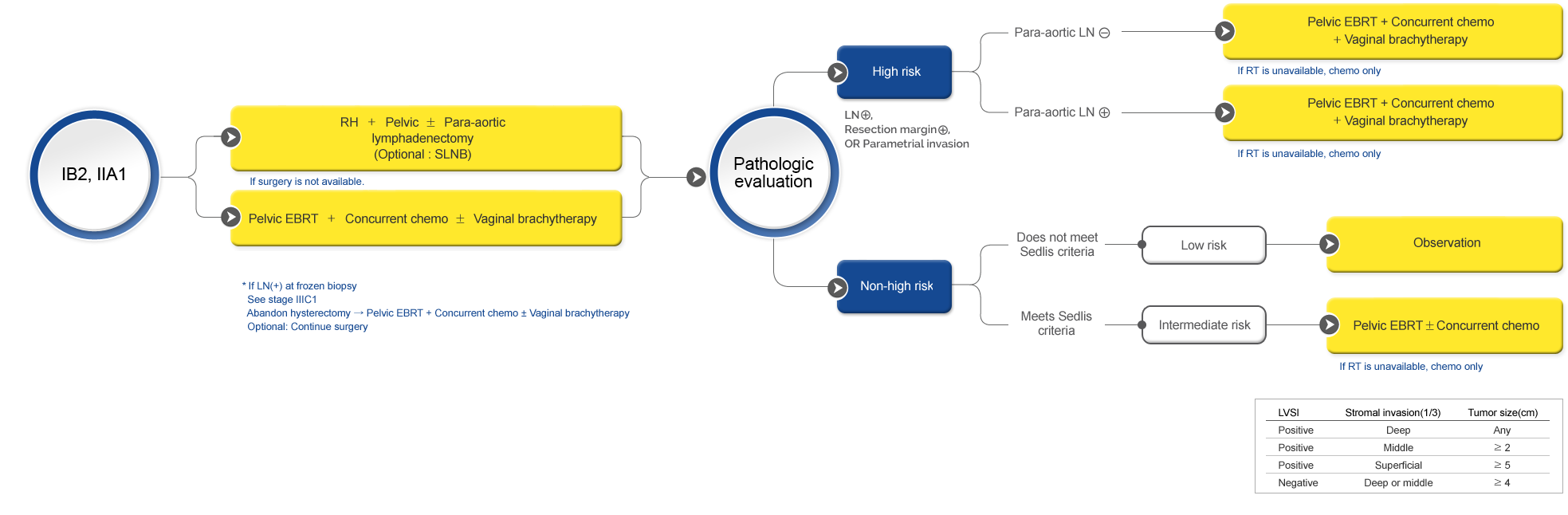
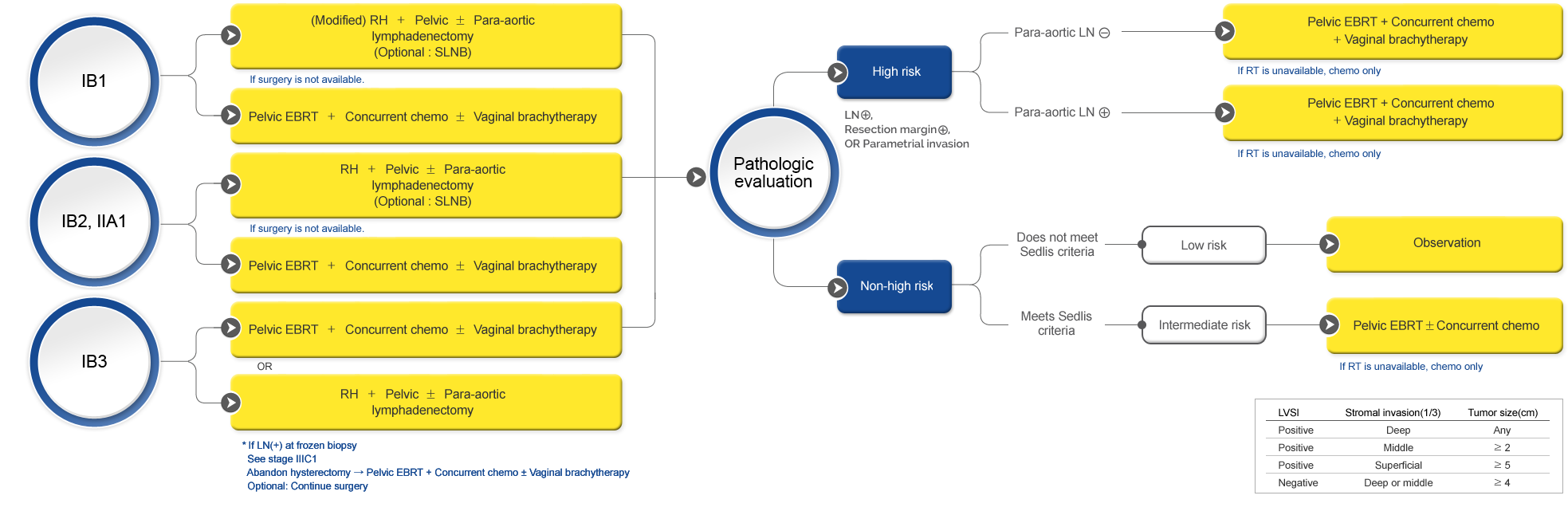
- The standard and recommended approach for RH is an open abdominal approach.
- For stage IB2-IIA disease, minimally invasive RH might be considered in research settings.
- The SHAPE trial is the only phase III RCT so far. According to the results, simple hysterectomy was not superior to RH in early-stage, low-risk cervical cancer.
- Simple hysterectomy may be considered a treatment option for stage IA2-IB1 disease.
- If SLNB is available and SLNs are negative, systemic lymphadenectomy can be omitted (no further nodal dissection).
- For SLNB, pathologic ultrastaging of SLNs is preferred to detect low-volume metastasis.
- If SLN mapping fails, side-specific LND should be performed. Bulky nodes should be removed.
- Neoadjuvant chemotherapy is not standard but can be considered in low-resource settings.